YOUR #1 CHOICE FOR
NYC PEST
CONTROL
Over 90 Years of commercial pest management within New York City, Long Island, Westchester County & Northern, NJ.





















































New York City Pest Control And Exterminators Serving NYC, Westchester County, Long Island, NY and Northern, NJ for Over 90 Years
Standard Pest Management has been solving New Yorkers pest problems since 1929. 2019 marks Standard’s 90th Year of setting the highest standards, established in 1929 we are the oldest pest control firm in New York City! Standard Pest Management is your New York Pest Control specialist.
Our mission is to provide effective professional pest control in New York city for all of our customers. We aim to improve the quality of life of our clients, community, environment and employees. We serve all types of customers from restaurant to retail and everything in between.
Learn More About Our Pest Control ServicesIndustries we provide Pest Management for

Exterminators In NYC, Westchester County, Long Island & Northern, NJ
Standard has been setting the “standard” in pest control and extermination in NYC for four generations. All commercial accounts are overseen by our Quality Control division. What that means for you is that there is a second level of attention given to your account’s pest control.
We also employ the latest technology to provide you with the most accurate reporting regarding areas treated, corrective measures, and reporting. Additionally, materials used are of the highest quality, used by licensed exterminators and pest control experts, in accordance with the label, all right here in New York City or Northern, NJ.
Learn More About Standarad Pest Management
When it comes to the differences between partnering with Standard vs another pest control company, i've always felt it important to emphasize just how important quality assurance is throughout every level of the service we provide. Our customers and their happiness has and will always be our number one priority."
 Josh BloomVP, Standard Pest Management
Josh BloomVP, Standard Pest Management
Need a Pest Management Expert in NYC?
Call, email, or fill out a quote request form for a fast and friendly quote today!


Get Your Quote Today!
In a hurry? Fill out our quick quote for a fast response.
Need a comprehensive estimate? Provide more info so we can reach back out with more insight.
Areas we Service
Best-In-Class Pest Control & Exterminating Services Throughout NYC
- New York City
- Manhattan
- Queens
- Brooklyn
- The Bronx
- Westchester County
- Nassau County
- Northern, New Jersey

Commercial Pest Management for Facilities in the New York City Metro Area
A pest problem within your business or commercial property can become a huge liability. Not only can it negatively impact your company image or brand, but pests can be a threat to customers, employees and vendors. When it comes to commercial pest management or extermination services in New York City, Standard is very well suited to meet your every need. We take a flexible, modern approach toward keeping unwanted bugs, rodents or birds away from your commercial premises.

Within warehouses and large storage facilities, bugs or rodents are often difficult to eliminate because they find clever hiding spots within hard-to-reach spaces. When our commercial exterminators visit an industrial client, we usually find pests that hide away inside shelving, tall ceilings, and even inside product boxes.
Since they’re looking for food, water and a cozy place to nest, they will look for the hardest to reach areas from your perspective to hide away. You can count on us for the very best in commercial pest management for just about every type of pest out there including bugs, flying insects, stinging insects, Rodents, nuisance Birds and wildlife.
Learn More About Commercial Pest ControlCommon Pests We Encounter & Your Treatment Options
-
 Ants
Ants
Formicidae
-
 Bedbugs
Bedbugs
Cimex lectularius
-
 Bees
Bees
Anthophila
-
 Birds
Birds
Aves
-
 Carpet Beetles
Carpet Beetles
Anthrenus verbasci
-
 Cockroaches
Cockroaches
Blattodea
-
 Fleas
Fleas
Siphonaptera
-
 Flies
Flies
Diptera
-
 Mosquitoes
Mosquitoes
Culicidae
-
 Webbing Clothes Moths
Webbing Clothes Moths
Lepidoptera
-
 Rodents
Rodents
Rodentia
-
 Spiders
Spiders
Araneae
-
 Spotted Lanternflies
Spotted Lanternflies
Lycorma delicatula
-
 Ticks
Ticks
Ixodida
-
 Termites
Termites
Isoptera
-
 Wildlife
Wildlife
Nuisance Animals
-
 Commercial Pest Control
Commercial Pest Control
Treatment & Protection for Your Business
-
 Residential Pest Management
Residential Pest Management
Treatment & Protection for Your Home
-
 Multi-Unit Apartment Pest Management
Multi-Unit Apartment Pest Management
Extermination From Apartments to Complexes
-
 Green Pest Management
Green Pest Management
Safe & Reduced Imprint on Your Environment
-
 Integrated Pest Management
Integrated Pest Management
All The Steps to Guarantee Satisfaction

Bird Control & Deterrent Solutions Throughout NYC & Long Island
Concerned about issues stemming from Birds? Don’t worry, you’ve come to the right place. At Standard Pest Management, we are your top choice within Manhattan, Queens, Brooklyn, The Bronx, Westchester or Northern, NJ for comprehensive bird control & deterrent installations. We’re not stating this just for the sake of stating it, we actually operate a 100% unique, specialized crew whose sole focus are to make bird problems disappear for our customers.
Most common nuisance bird species such as Pigeons, Sparrows, Starlings or Seagulls might not seem like such a scary threat at first impression. Flocks start to become a much greater problem if your commercial property is without protection, serves a reasonable amount of foot traffic in the form of customers and employees. There are a wide range of liabilities to be concerned with because all are very real possibilities.

Birds can cause all kinds of headaches 24 hours a day, 7 days a week directly on your property. Droppings are not only a terrible eyesore, they are also highly acidic which means you’ll have to worry about refinishing or replacing exterior building materials and they carry disease. Their droppings along with nesting materials, feathers and any other elements they continue to bring back to their nest on a daily basis become a haven for disease, parasites and a host of other problems.
We provide just about every major facet of bird control and clean-up for any customer across all verticals or industries within New York. From the cleaning & disinfecting solutions we provide for those with bird dropping issues to highly customized deterrent solutions formulated to keep birds out of your property and even lower population count, we have got you covered. We only practice time-tested, industry standard techniques, have decades of experience, and really focus on becoming the last stop for any bird control solutions you may need.
Learn More About Bird Control & DeterrentsOnly the Most Effective & Proven Deterrents for Bird Flocks Available
-
Bird Control & Removal
Ares
-
 Pigeon Control & Removal
Pigeon Control & Removal
Columbidae
-
 Sparrow Control & Removal
Sparrow Control & Removal
Passeridae
-
 Starling Control & Removal
Starling Control & Removal
Sturnidae
-
 Seagull or Seabird Control & Deterrent Options
Seagull or Seabird Control & Deterrent Options
Larinae
-
 Bird Netting
Bird Netting
Perfect for the Largest of Spaces
-
 Bird Spikes
Bird Spikes
Highly Flexible Installation
-
 Bird Wire
Bird Wire
Time Tested & Durable
-
 Electric Shock System
Electric Shock System
Effective & Out of Sight
-
 Optical Gel Multi-Sensory Bird Repellent
Optical Gel Multi-Sensory Bird Repellent
Birds Hate Sticky Surfaces
-
 Balcony or Terrace Bird Control & Prevention in New York City
Balcony or Terrace Bird Control & Prevention in New York City
Keep Birds Off Your Balcony
-
 OvoControl Flock Management
OvoControl Flock Management
Reduce Bird Populations
-
 Bird Dropping Cleanup
Bird Dropping Cleanup
Pressure Washing & Disinfectant

Fly Treatment & Control Services in New York City
Unfortunately, swatting flies with a newspaper is only a temporary solution to a far more persistent problem. The only way to get rid of them is by making sure their presence in the home of commercial facility is being managed by an experienced pest management company. You’re not just looking at a nuisance, but possible health issues when it comes to flies. Standard will help remove and prevent further infestations of the common house fly, drain flies, fruit flies, blow flies and gnats so you can go about your day in peace.

It is essential to deal with the infestation as soon as you notice them avert a crisis. The best way to ensure that you get rid of these annoying creatures is to get help from a reputable drain fly cleaning and extermination company.
You can rely on Standard Pest Management for fly control in the New York Metropolitan area and NJ. We know how quickly a housefly infestation can escalate, which is why we offer meticulous and practical solutions.
Learn More About Fly Treatment & Control

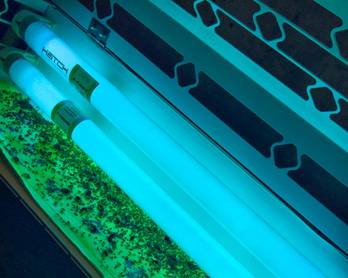
UV Fly Trap Installation for Your Facility or Property
Of all the different available methods of removing sewer flies, UV traps are some of the most successful. At specific wavelengths, UV rays are irresistible to fruit flies. These traps are therefore created to attract the houseflies and then trap them onto sticky surfaces. Once they are caught, all that remains is to discard them. Over time, the housefly population in your property will dwindle until there are no more of these annoying insects left.
There are various types of UV fly traps that can be used to catch houseflies. The first is a wall-mounted trap. Typically, this Insect Light Trap is mounted within 5 feet of the floor. For narrow spaces such as hallways where a wall-mounted trap would be a bother, a ceiling mount is used instead. If the housefly nuisance is present in public areas, you can use decorative wall sconces to deal with the problem discreetly.